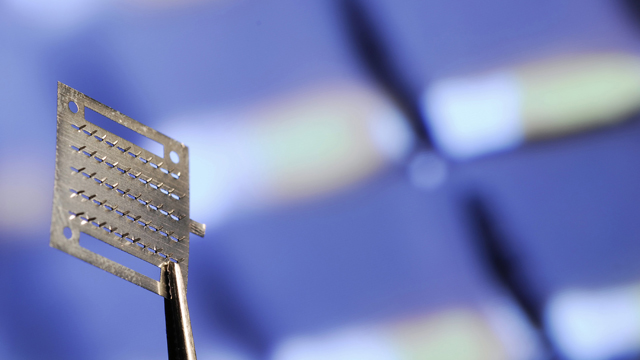
 An array of microneedles can be coated with medicine and act as a painless drug delivery system for vaccines EMORY UNIVERSITY
An array of microneedles can be coated with medicine and act as a painless drug delivery system for vaccines EMORY UNIVERSITY
THE DEVICE: In the near future, your annual flu shot may not be a sharp jab in the arm but a sticky, spiny band-aid applied gently to your skin. Over the past five years, researchers at Emory University and the Georgia Institute of Technology have developed a dime-sized vaccine patch sprinkled with a hundred microscopic needles and coated with a vaccine solution. The patch, which could someday be self-administered, comes in two versions: metal or dissolvable polymer. It has successfully protected mice from influenza, and now researchers know exactly how the tiny microneedles elicit an immune response in the skin.
WHAT’S NEW: In 2011, the Emory-Georgia team demonstrated vaccine delivery via microneedle patches is often more protective than inoculation under the skin or into muscle, ...












